71% of haemodialysis patients arrive overhydrated for every session.
Not slightly elevated. Not borderline. They carry clinically significant excess extracellular fluid. This fluid silently raises blood pressure. It also stretches the left ventricle and impairs lung function. Over time, it accelerates cardiovascular disease.
However, the most alarming part is not the prevalence.
It is the fact that most cases go undetected. Nephrologists and dialysis nurses still rely on clinical assessment. They also depend on weight-based dry weight targets. These methods simply cannot detect hidden fluid overload.
Hidden fluid overload in dialysis patients is one of the most studied problems in nephrology. Yet, it remains under-managed. The evidence is clear. Excess extracellular water (ECW) significantly increases mortality risk.
A post-dialysis ECW/TBW ratio above 0.5023 is strongly linked to poor outcomes. Studies show mortality rates of 69.6% over 30 months (PMC, 2021). This is more than double the risk seen in patients with normal fluid levels.
In this article, we highlight seven critical mistakes.
These mistakes allow hidden fluid to sabotage dialysis outcomes. We also explain how InBody BIA-guided fluid management helps prevent each one.
| 71% Haemodialysis patients overhydrated before every session (PMC 2025) | 69.6% 30-month mortality in HD patients with post-dialysis ECW/TBW above 0.5023 (PMC 2021) | 43% Of dialysis deaths caused by cardiovascular events directly driven by fluid overload | 5 min Time for InBody S10 bedside body composition and fluid assessment in lying-down dialysis patients |
The Hidden Fluid Problem: Why Weight Alone Cannot Find It
Dry weight refers to the target body weight after dialysis, where the patient reaches fluid balance. It forms the cornerstone of dialysis adequacy. However, the challenge lies in how clinicians set it. Most dialysis centres still rely on clinical assessment. They check blood pressure, look for oedema, assess dyspnoea, and review the patient’s pre-dialysis weight. However, these methods have one major limitation. They cannot distinguish between fluid and body tissue.
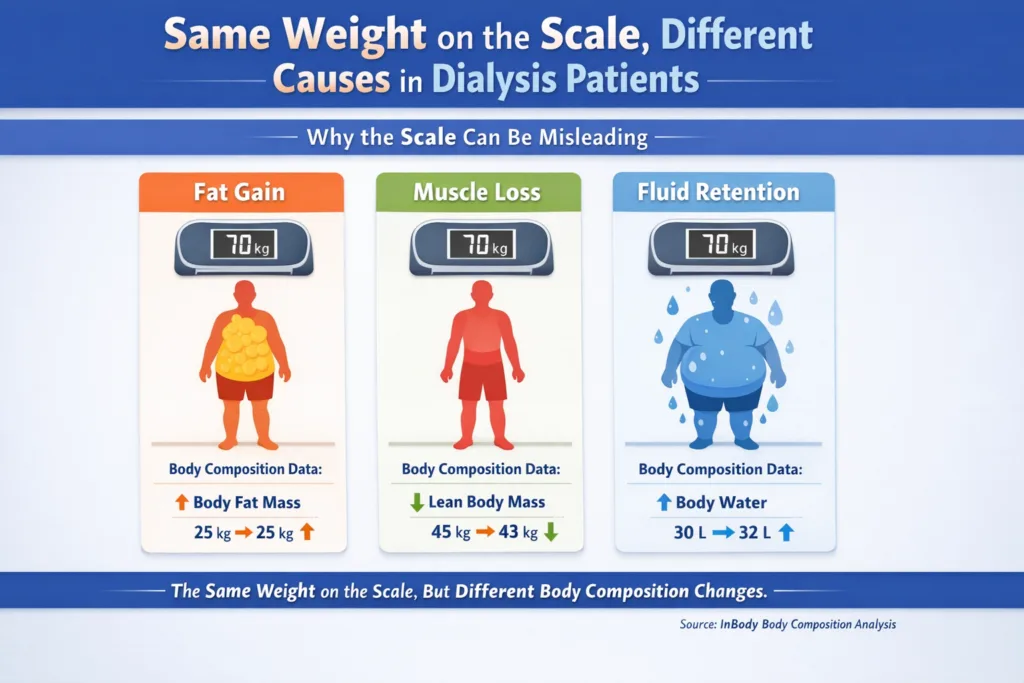
A dialysis patient who gains 2 kg of adipose tissue over 6 months while losing 1.5 kg of skeletal muscle, common in dialysis-related sarcopenia, may appear at their dry weight by scale measurement while carrying significant hidden fluid overload. Their weight has changed, body composition has deteriorated. Their dry weight target is wrong. And without direct body composition measurement, no one knows.
THE CLINICAL BLIND SPOT
Clinical assessment of fluid overload inspection, percussion, blood pressure, and body weight has a sensitivity as low as 30–50% for detecting pre-dialysis overhydration at clinically relevant levels. A patient can be carrying over 2 litres of excess extracellular fluid and present without oedema or respiratory symptoms. Only bioelectrical impedance analysis (BIA) measures ECW directly and quantifies the overload.

Mistake 1: Relying Solely on Weight to Set Dry Weight Targets
Weight-based dry weight assessment cannot differentiate fluid from fat or lean tissue. When a dialysis patient’s body composition changes, fat accumulates, and muscle mass decreases. As a result, their true euvolaemic weight changes independently of their scale weight. If clinicians rely only on scale weight to set dry weight targets, they set inaccurate targets for patients experiencing body composition changes. In dialysis populations, almost every patient goes through these changes over time.
A 2022 BMC Nephrology study compared the InBody 770 and InBody S10. The researchers found that ECW/TBW-based BIA accurately estimated target weights. These estimates showed a near-perfect correlation (R² = 1.0) between the devices. They also observed that BIA-derived targets differed from clinically set weight-based targets. This difference was more noticeable in patients on long-term dialysis and in those with diabetes-related changes in body composition.
CLINICAL IMPLICATION
Dry weight should be reassessed using BIA-derived ECW/TBW data at a minimum every 3 months and immediately after any significant clinical change (hospitalisation, infection, dietary change, body weight change of more than 2 kg). InBody S10 delivers this assessment in under 5 minutes in the lying-down dialysis position without requiring the patient to stand or transfer from the bed.
Mistake 2: Missing Fluid Overload That Presents Without Oedema or Symptoms
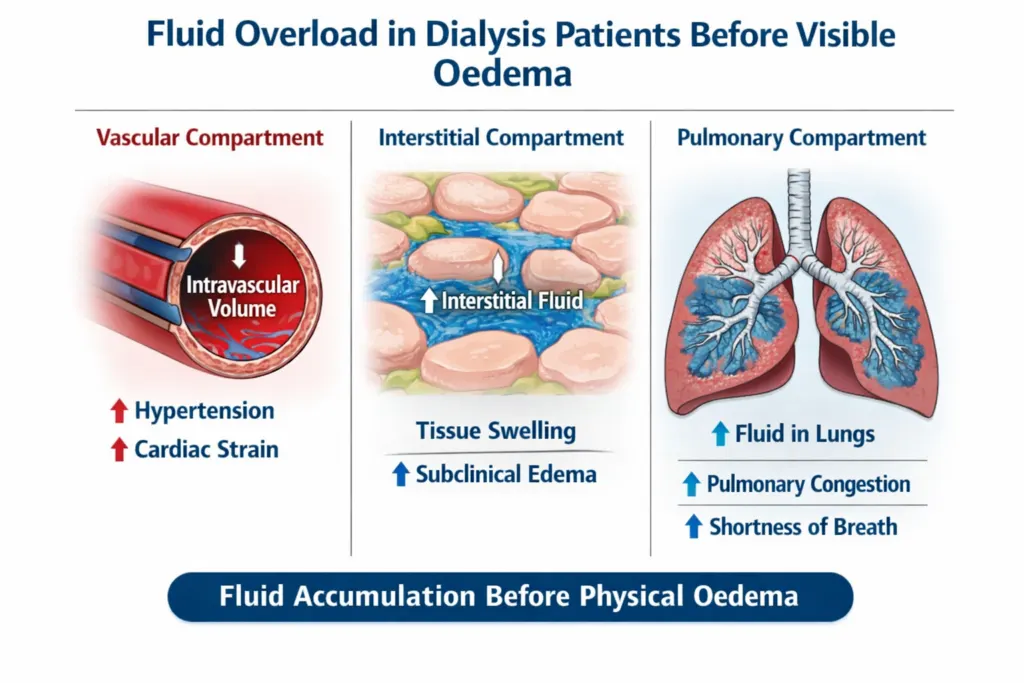
The clinical myth that fluid overload always shows up as visible oedema is one of the most dangerous assumptions in dialysis care. Extracellular fluid spreads across multiple compartments, including vascular, interstitial, and third-space areas. As a result, significant overhydration can build up in visceral and pulmonary compartments before clinicians notice any peripheral oedema.
A 2025 PMC study found that 71% of patients had overhydration before dialysis. Importantly, many of these patients showed no visible oedema during clinical examination. After a 4-hour haemodialysis session, many patients still had excess fluid despite significant removal. Moreover, this persistent overhydration directly impaired lung function, reduced FEV1 and FVC, increased blood pressure, and affected endothelial function markers.
KEY INSIGHT
The PLOS ONE 2017 multicenter study confirmed that ECW overload in haemodialysis patients is independently associated with elevated VCAM-1 (a marker of endothelial dysfunction) even after controlling for age, comorbidity, and dialysis intensity. Endothelial damage from persistent hidden fluid overload progresses silently, measurable only through serial BIA assessment of ECW/TBW ratio.
Mistake 3: Not Measuring ECW/TBW Ratio as a Mortality Predictor
The ECW/TBW ratio is the most clinically validated BIA-derived marker for predicting mortality in dialysis patients. However, most Indian dialysis centres do not measure it. Instead, clinicians routinely monitor blood pressure, haemoglobin, Kt/V adequacy, and serum albumin. ECW/TBW, a direct measurement that costs nothing beyond the initial BIA device investment and takes 5 minutes, is not.
The evidence for its predictive value is compelling. A multicenter prospective study found that post-dialysis ECW/TBW was directly associated with NT-proBNP and cTnT established cardiovascular biomarkers and that patients with post-dialysis ECW/TBW above 0.5023 had a mortality rate of 69.6% over 30 months, compared to 32.4% in those below this threshold. The KDOQI Nutrition Guidelines in CKD have already suggested using post-dialysis bioimpedance to assess body composition in adults with CKD 5D on maintenance haemodialysis.
THE ECW/TBW MORTALITY THRESHOLD
Normal post-dialysis ECW/TBW range: 0.390–0.406
High-risk threshold: above 0.4713 (75% of HD patients in one study exceeded this)
Critical mortality threshold: above 0.5023 (independently associated with 69.6% all-cause mortality at 30 months)
InBody S10 measures ECW/TBW at every session. Without this measurement, you are managing fluid blindly against the single most predictive mortality marker in your dialysis population.
Mistake 4: Confusing Body Weight Change With Fluid Change
In dialysis populations, body weight change has three possible sources: fluid change, fat mass change, and lean tissue change. Weight-based assessment assumes that interdialytic weight gain is entirely fluid but this is only valid if body composition is static. It never is.
A 2023 Scientific Reports prospective study of haemodialysis patients followed over 20 months found that despite adequate ultrafiltration, the overhydration (OH) parameter significantly increased over time. This increase was driven not by rising ECW alone, but by a simultaneous significant decline in intracellular water (ICW) reflecting progressive muscle loss. Patients whose ICW was below 17 L had significantly elevated all-cause mortality (Kaplan–Meier, p = 0.018), confirming that hidden muscle loss, not just fluid overload, is silently contributing to the clinical picture that weight monitoring cannot capture.
CLINICAL IMPLICATION
Every significant body weight change in a dialysis patient should be investigated with a BIA measurement before adjusting the dry weight target. A patient who has lost 2 kg over 3 months may have lost lean tissue, not fluid, making their current dry weight target already too low. Conversely, a patient who has gained 2 kg in the same period may have gained adipose tissue, not fluid, making their target too high. Only BIA can tell you which it is.
Mistake 5: Ignoring Persistent Post-Dialysis Overhydration
Many dialysis units measure fluid status only pre-dialysis and use the difference between pre- and post-dialysis weight as the sole measure of fluid removal adequacy. This misses the most clinically important measurement: whether the patient is actually euvolaemic after the session.
The 2025 PMC study found that many patients remained overhydrated even after a complete 4-hour haemodialysis session, confirmed by BIVA analysis, showing most participants still in the overhydration quadrant post-dialysis. This persistent post-dialysis overhydration was directly associated with impaired spirometry results: reduced FEV1, FVC, and PEFR markers of pulmonary congestion that clinical examination may not detect until they are severe.
Post-dialysis BIA measurement is the only way to confirm that euvolaemia has been achieved. Without it, ultrafiltration targets are based on a weight goal, not a fluid goal. The distinction matters clinically, especially in patients with diabetes, cardiac disease, or significant sarcopenia where body composition is most likely to have shifted from the assumed norm.
Mistake 6: Failing to Monitor the Fluid–Nutrition Relationship in Dialysis Malnutrition
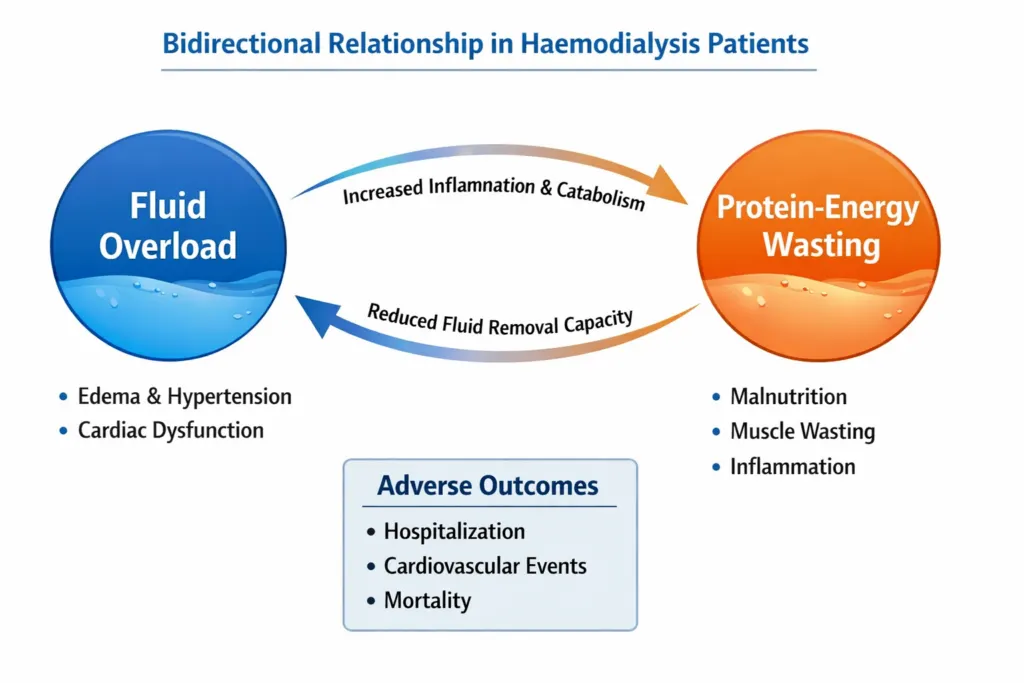
Fluid overload and malnutrition are not independent problems in dialysis patients; they are deeply intertwined. A 2023 Scientific Reports study confirmed that an elevated ECW/TBW ratio in haemodialysis patients is independently associated with protein-energy wasting (PEW), lower serum albumin, lower normalised protein catabolic rate (nPCR), and lower serum creatinine. This means that a dialysis patient who is both malnourished and overhydrated will have a severely elevated cardiovascular mortality risk that is substantially higher than either problem alone.
The mechanism is bidirectional. Malnutrition drives muscle loss, which reduces ICW and raises the ECW/TBW ratio. Fluid overload drives inflammation through elevated VCAM-1 and IL-6, which accelerates further muscle catabolism through inflammatory myopathy. Without measuring both ECW/TBW ratio and lean tissue index simultaneously, which InBody S10 does at every session, this deadly interaction is invisible to the clinical team.
KEY INSIGHT
The Scientific Reports 2023 study confirmed that adding ECW/TBW ratio data to a standard protein-energy wasting (PEW) score in haemodialysis patients significantly improved the C-index and net reclassification improvement for mortality prediction. In other words, BIA-derived fluid data is independently predictive of mortality above and beyond conventional nutritional assessment tools.
Mistake 7: Not Using BIA to Guide Fluid Management Protocols
The most dangerous mistake of all is also the most preventable: not implementing BIA-guided fluid management despite the availability of validated tools, published protocols, and compelling mortality data. A 2024 ScienceDirect randomised controlled trial of critically ill post-operative patients showed that BIA-guided fluid management using ECW/TBW ratio to titrate ultrafiltration produced a 28-day mortality rate of 1.3%, compared to 14.4% in patients managed with traditional clinical assessment alone (p = 0.002).
For dialysis patients, the evidence is equally clear. KDOQI guidelines now recommend post-dialysis BIA for body composition and fluid status assessment. The Indian Consensus on Sarcopenia (2025) recommends BIA for all patients with CKD 5D (maintenance dialysis). Multiple published RCTs confirm that BIA-guided dry weight setting reduces intra-dialytic hypotension, improves blood pressure control, and reduces left ventricular mass index independent of pharmacological intervention.
WHY THIS IS STILL NOT STANDARD IN INDIA
Despite the evidence, BIA-guided fluid management remains the exception rather than the standard in Indian dialysis centres. The barrier is not clinical evidence; the evidence is unambiguous. The barrier is device availability and workflow integration. InBody S10 was specifically engineered to remove both barriers. It operates in the lying-down dialysis position, delivers results in under 5 minutes, and requires no additional patient transfer or preparation beyond what is standard in routine dialysis care.
What the InBody S10 Measures in Dialysis Patients
The InBody S10 is the InBody device specifically validated for bedside body composition and fluid management in dialysis, critically ill, and non-ambulatory patients. Unlike standard InBody devices that require standing, the S10 is designed to be used in the lying position, allowing pre-dialysis, intra-dialytic, and post-dialysis measurement without disturbing the patient or the session.
| InBody S10 Metric | What It Measures | Clinical Application in Dialysis |
|---|---|---|
| ECW/TBW Ratio | Extracellular water as a proportion of total body water | Primary fluid status marker tracks overhydration, guides dry weight setting, and predicts mortality |
| Overhydration Index (OH) | Litres of excess ECW above the calculated normal | Quantifies the absolute fluid burden and guides ultrafiltration volume targets |
| Total Body Water (TBW) | Total fluid volume in the body | Tracks fluid balance trends across sessions and over time |
| Extracellular Water (ECW) | Fluid outside cells plasma and interstitial fluid | The primary overhydration compartment directly reflects the fluid overload burden |
| Intracellular Water (ICW) | Fluid inside cells reflects muscle mass and nutritional status | ICW below 17 L independently associated with mortality (Scientific Reports 2023) |
| Lean Tissue Index (LTI) | Lean mass normalised for height tracks muscle | Detects dialysis-related sarcopenia concurrent with fluid assessment |
| Fat Tissue Index (FTI) | Fat mass normalised for height tracks adiposity | Identifies sarcopenic obesity, high FTI combined with low LTI, and elevated ECW/TBW |
Real Case: The Dialysis Patient Whose Dry Weight Was Wrong for 18 Months
A 58-year-old male patient with ESRD secondary to diabetic nephropathy had been on maintenance haemodialysis for 3 years at a centre in Chennai. His dry weight was 68 kg, set clinically 18 months earlier and not reviewed since. His blood pressure was persistently elevated at 158/94 mmHg despite three antihypertensive agents. He had experienced two episodes of intra-dialytic hypotension in the preceding 6 months. His nephrologist suspected his dry weight target was too low.
So his first InBody S10 assessment performed in the lying position immediately after a dialysis session told a completely different story; the post-dialysis ECW/TBW ratio was 0.487 (well above the 0.406 normal upper limit), and His overhydration index was +1.8 L, confirming he was still significantly overloaded after what appeared to be an adequate session. His LTI was below population norm, and his FTI had increased since his last clinical review, confirming fat accumulation concurrent with muscle loss over the 18 months since his dry weight was set.
After 12 weeks of BIA-guided dry weight adjustment, incrementally reducing his target weight and titrating ultrafiltration volumes using serial InBody S10 data, his outcomes showed the following changes:
| ↓0.038 ECW/TBW ratio improvement (0.487 → 0.449) | ↓1.2 L Overhydration index reduction | ↓16 mmHg Systolic BP reduction at 12 weeks | Zero Intra-dialytic hypotension episodes in 12-week period |
His antihypertensive regimen was subsequently reduced from three agents to two. His nephrologist attributed the blood pressure improvement almost entirely to the correction of persistent hidden fluid overload fluid that weight-based assessment had been missing for 18 months.
Frequently Asked Questions
Q. What is fluid overload in dialysis patients?
Fluid overload in haemodialysis patients occurs when excess extracellular water (ECW) accumulates between dialysis sessions, expanding the extracellular fluid compartment beyond normal limits. It is the most common and dangerous complication of dialysis associated with hypertension, left ventricular hypertrophy, heart failure, lung impairment, endothelial dysfunction, and significantly elevated cardiovascular mortality. Studies confirm that 71% of patients arrive overhydrated before each dialysis session.
Q. How does hidden fluid affect dialysis outcomes?
Hidden fluid overload causes hypertension, left ventricular hypertrophy, endothelial dysfunction, impaired lung function (reduced FEV1 and FVC), accelerated cardiovascular disease progression, protein-energy wasting, and elevated all-cause mortality. Dialysis patients with post-dialysis ECW/TBW above 0.5023 have been shown to have a 69.6% mortality rate over 30 months versus 32.4% in well-hydrated patients. The majority of this excess mortality is driven by cardiovascular events (43% of deaths in published series).
Q. How does InBody S10 help manage fluid in dialysis patients?
The InBody S10 was specifically designed for bedside body composition assessment in dialysis and non-ambulatory patients. It measures ECW, TBW, ICW, ECW/TBW ratio, overhydration index (OH in litres), lean tissue index (LTI), and fat tissue index (FTI) in under 5 minutes in the lying position without requiring the patient to stand or transfer from the dialysis chair or bed. This data enables nephrologists to set accurate dry weight targets, detect persistent post-dialysis overhydration, identify fluid trends over serial sessions, and differentiate fluid gain from tissue changes, none of which scale-based assessment can achieve.
Key Takeaways
- 71% of haemodialysis patients arrive overhydrated before every session, and most of this fluid overload is invisible to clinical assessment and weight-based dry weight monitoring.
- The 7 dangerous mistakes relying on weight for dry weight, missing asymptomatic overload, ignoring ECW/TBW mortality data, confusing weight change with fluid change, ignoring post-dialysis overhydration, missing the fluid–nutrition interaction, and not using BIA protocols all have the same root cause: not measuring ECW directly.
- Post-dialysis ECW/TBW ratio above 0.5023 is independently associated with 69.6% all-cause mortality over 30 months more than double the mortality in euvolaemic patients. This is the single most important number in dialysis care that most centres are not measuring.
- InBody S10 measures ECW, TBW, overhydration index, ECW/TBW ratio, LTI, and FTI in under 5 minutes in the lying position providing the complete fluid and body composition picture that weight-based assessment cannot deliver, without disrupting the dialysis session.
- KDOQI guidelines now recommend post-dialysis bioimpedance for body composition assessment in CKD 5D patients. The Indian Consensus on Sarcopenia (2025) recommends BIA for all patients with maintenance dialysis. The clinical evidence for InBody S10-guided fluid management is no longer emerging it is established.
- BIA-guided fluid management in a 2024 RCT produced a 28-day mortality rate of 1.3% versus 14.4% in controls (p = 0.002) confirming that the mortality benefit of ECW/TBW-guided protocols is clinically significant and immediately achievable.
Stop Managing Fluid Blindly
InBody S10 delivers bedside ECW/TBW ratio, overhydration index, and complete body composition data for every dialysis patient in under 5 minutes, in the lying position, at every session. Available for Indian dialysis centres, nephrology units, and intensive care facilities.

Find an InBody Scanner Near You
References & Further Reading
- PMC 2025. Persistent overhydration despite fluid reduction after haemodialysis — BIA/BIVA study. PMC12686928.
- PMC 2021. ECW/TBW ratio as predictor of mortality in haemodialysis patients — multicenter prospective study. PMC8118427.
- Scientific Reports 2023. ECW/TBW ratio association with protein-energy wasting and mortality in haemodialysis patients. Nature.
- ScienceDirect 2024. BIA-guided fluid management RCT in critically ill patients — ECW ratio 28-day mortality outcome.
- PMC 2020. Low ICW, overhydration, and mortality in haemodialysis patients — 124 patient prospective study. PMC7697083.
- PLOS ONE 2017. Extracellular overhydration linked with endothelial dysfunction in haemodialysis CKD. PLOS ONE.
- BMC Nephrology 2022. InBody 770 vs InBody S10 — ECW/TBW and target weight consistency in HD patients. BMC Nephrology.
- Kalra S et al. Indian Consensus on Sarcopenia including CKD 5D recommendations. Int J Gen Med. 2025;18:1731–1745.